
Gastric Sleeve vs. SADI-S vs. GLP-1 Medications
A 2026 Comparison Guide for Patients in Houston, TX
Medically Reviewed By
Dr. Ricardo M. Bonnor, MD, FACS, FASMBS
Board Certified — American Board of Surgery | American Board of Cosmetic Surgery
Fellow American College of Surgeons (FACS)
Fellow American Society for Metabolic and Bariatric Surgery (FASMBS)
Member, American Society of Metabolic and Bariatric Surgery (ASMBS)
20+ years experience | 10,000+ cases (primary, revisional, laparoscopic & robotic)
Hospital Affiliations: Memorial Hermann Kingsland Surgery Center (MBSAQIP accredited Center of Excellence) Director of Ambulatory Bariatric Surgery- Memorial Hermann Kingsland Surgery Center| Staff Member Memorial Hermann Memorial City Hospital
Texas Aesthetics & Bariatrics — 18211 Katy Freeway, Suite 250, Houston, TX 77094
Insurance Accepted: Aetna, United Healthcare, Cigna, Blue Cross Blue Shield (BCBS)
Quick Answer
Gastric sleeve, SADI, and GLP-1 medications each address obesity and metabolic disease in different ways and at different levels of intensity. A gastric sleeve removes about 80% of the stomach to limit how much you eat. A SADI-S which stands for single anastomosis duodenal-ileal bypass with sleeve gastrectomy is a sleeve (S) with an intestinal bypass (SADI), so it limits both how much you eat and how many calories you absorb. You may also see other terms for SADI-S such as “loop DS” or “single anastomosis duodenal switch”. The accepted clinical term is now SADI-S. The sleeve is simpler with fewer nutritional risks. SADI-S delivers greater long-term weight loss and stronger control of type 2 diabetes, making it a strong option for higher BMIs and for patients who have regained weight after a prior sleeve. SADI-S has a higher nutritional risk due to the intestinal component.
GLP-1 medications are effective while you take them, but weight returns when you stop. GLP-1 medication is typically indicated for lower BMI patients but may also carry nutritional risk such as poor protein body composition relative to fat mass.
For patients in Houston, TX, Dr. Ricardo Bonnor performs both sleeve and SADI-S surgery and helps patients determine which path either surgical or staged is right for their specific health profile. Dr Bonnor also prescribes GLP-1 medication under a physician supervised program which includes body composition analysis. We accept Aetna, United Healthcare, Cigna, and BCBS.
A self-pay sleeve gastrectomy starts at $9,900 with financing available.
For readability, the rest of this article uses SADI to refer to the SADI-S procedure.
More patients than ever are weighing their options when it comes to serious, lasting weight loss. The conversation used to be straightforward. Now there are three meaningful paths on the table: gastric sleeve surgery, SADI surgery, and GLP-1 medications like semaglutide and tirzepatide. Since SADI-S is a sleeve with an intestinal bypass, the article will address a sleeve vs SADI VS GLP-1.
At Texas Aesthetics & Bariatrics in Houston, TX, Dr. Ricardo Bonnor performs both gastric sleeve surgery and SADI surgery, and understands the GLP-1 landscape = to speak honestly about where medication fits and where it falls short. Patients receive recommendations based on their medical profile.
Side-by-Side: Gastric Sleeve vs. SADI vs. GLP-1 Medications
The table below provides a direct clinical comparison across the three options. The sections that follow explain each row in plain language.
| Feature | Gastric Sleeve | SADI (Sleeve + Intestinal Bypass) | GLP-1 Medications |
| Mechanism | Restriction + ghrelin reduction | Restriction + malabsorption + hormonal | Pharmacological appetite suppression |
| Stomach change | 75–80% permanently removed | 75–80% removed (same as sleeve) | None — anatomy unchanged/td> |
| Intestinal change | None | Single anastomosis to ileum | None |
| Average weight loss | 60–70% excess body weight | 70–90% excess body weight | 10–15% total body weight (on medication) |
| Durability | Permanent anatomical change | Permanent anatomical change | Weight returns ~18 months after stopping† |
| Type 2 diabetes | Significant improvement | Up to 60%+ remission; 3.48× higher odds vs RYGB‡ | Significant while on medication |
| GERD / reflux | May worsen in some patients | Pyloric valve preserved; lower reflux risk | Neutral to mild worsening |
| Nutritional needs | Standard bariatric vitamins | Enhanced: vitamins A, D, E, K, B12, iron, zinc | Standard multivitamins |
| Cost structure | One-time investment | One-time investment | Ongoing monthly cost; ~$11,689 more than surgery over 2 years§ |
| Reversibility | Permanent | Intestinal portion reversible | Fully reversible — stop medication |
| Ideal candidate | BMI 35–49; earlier metabolic disease | BMI 50+; advanced T2D; prior sleeve inadequate | BMI ≥27–30; earlier intervention or bridge to surgery |
† Berg et al., Obesity Reviews, 2025. ‡ Sabatella et al., Obesity Surgery, 2025. § Barrett et al., JAMA Surgery, 2025. See Clinical References.
Understanding GLP-1 Medications (Semaglutide & Tirzepatide)
GLP-1 receptor agonists work by mimicking gut hormones that signal fullness to the brain, slow stomach emptying, and reduce appetite. They do not change the anatomy of the stomach or intestines.
In clinical trials, GLP-1 medications produce meaningful weight loss typically 15 to 21% of total body weight. For many patients, that is a significant and life-changing result. But there are important limitations that patients need to understand before choosing this path.
The Durability Problem
GLP-1 medications only work while you are taking them. When patients stop, the weight comes back. A 2025 systematic review and meta-analysis (Berg et al., Obesity Reviews) found that patients stopping semaglutide or tirzepatide regained a mean of 9.69 kg, with regain proportional to how much was originally lost. University of Oxford research confirms that most patients return to their pre-treatment weight within approximately 18 months of stopping.
The Discontinuation Reality
According to data from the ASMBS 2025 Annual Scientific Meeting, up to 70% of patients stop taking GLP-1 medications within one year which is most commonly due to cost, insurance coverage gaps, or gastrointestinal side effects. This makes the real-world durability of GLP-1 therapy considerably lower than clinical trial numbers suggest.
The Long-Term Cost
GLP-1 medications are an ongoing monthly expense. A 2025 study published in JAMA Surgery (Barrett et al.) found that over two years, patients on GLP-1 therapy spent approximately $11,689 more than patients who had bariatric surgery.. For patients who take GLP-1 medications for five, ten, or twenty years, the cumulative expense is substantial.
When GLP-1 Medications Make Sense
GLP-1 medications are a legitimate and effective option for many patients particularly those who are not yet candidates for surgery, prefer a non-surgical approach, or want to lose weight before surgery to reduce operative risk. They can also serve as a bridge to surgery for patients who want to make progress while preparing for a more permanent intervention. Dr. Bonnor does not dismiss GLP-1 therapy. He helps patients understand where it fits in their specific journey.
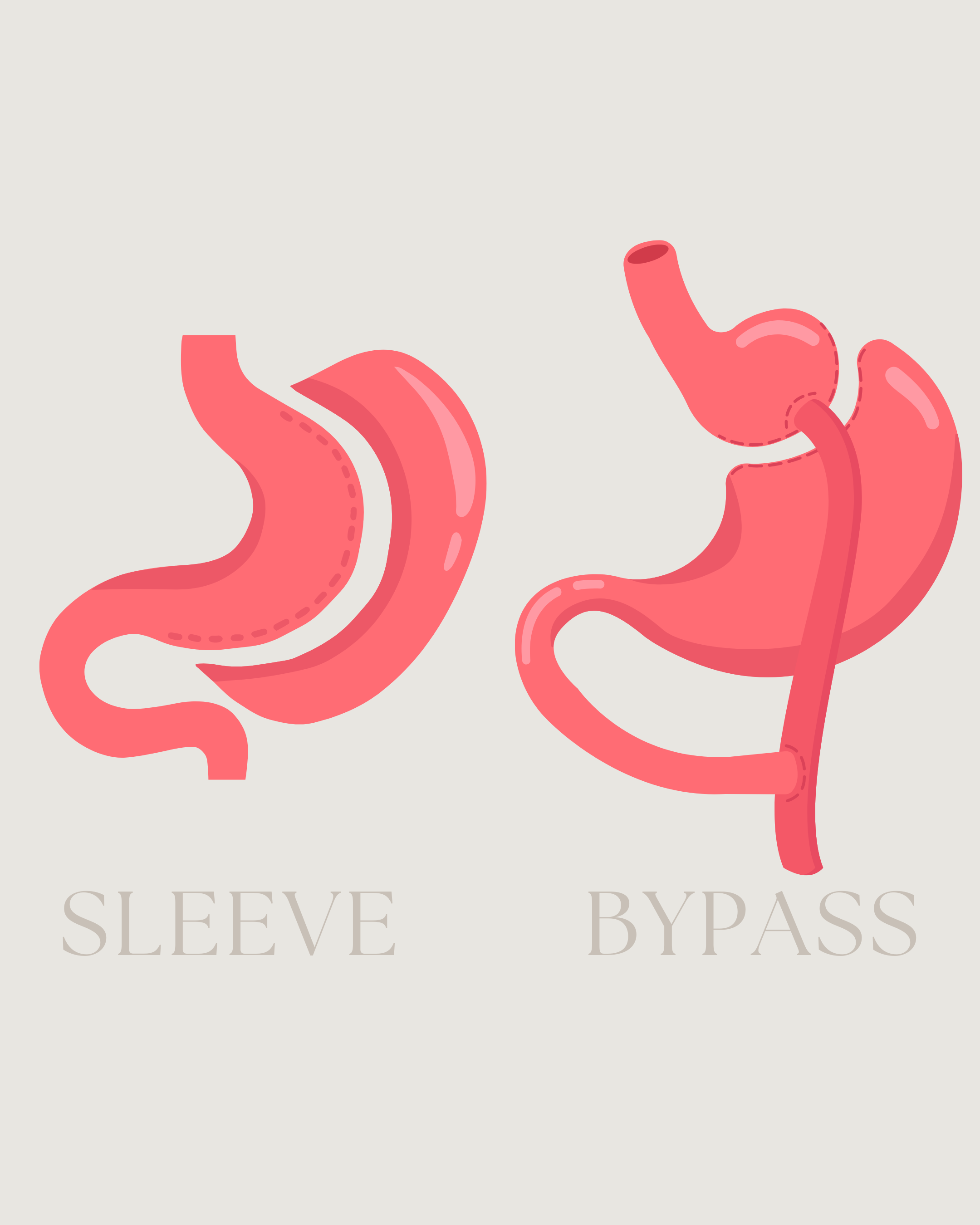
Understanding Gastric Sleeve Surgery
Gastric sleeve surgery permanently removes approximately 75 to 80% of the stomach, leaving a narrow, tube-shaped pouch. Unlike GLP-1 medications, gastric sleeve surgery creates a structural change that does not require ongoing treatment to maintain its effect.
Gastric sleeve surgery produces approximately 60 to 70% excess body weight loss in the first 12 to 18 months, with durable long-term results. It also improves or resolves many obesity-related conditions including type 2 diabetes, high blood pressure, sleep apnea, and joint pain.
Who Sleeve Surgery Is Best For
Gastric sleeve is generally best suited for patients with a BMI in the 30 to 49 range, earlier-stage metabolic disease, and a preference for a straightforward digestive anatomy after surgery. It is also a natural next step for patients who have plateaued or stopped GLP-1 medications and want a more permanent solution.
One important consideration: a small number of patients experience worsening acid reflux (GERD) after sleeve surgery because the procedure removes the fundus of the stomach, which can affect the lower esophageal sphincter. Patients with existing GERD should discuss this carefully with Dr. Bonnor during consultation.
Understanding SADI Surgery
SADI or single anastomosis duodenal-interposition is best understood as a gastric sleeve plus an intestinal bypass. It includes everything sleeve surgery does and then adds a single surgical connection between the duodenum and the lower small intestine. This intestinal bypass creates a powerful malabsorptive component that dramatically amplifies both weight loss and metabolic outcomes.
Because SADI uses a single intestinal connection rather than the two required in traditional gastric bypass, it is considered technically simpler than Roux-en-Y bypass while delivering comparable and in recent studies, superior results. The landmark SADISLEEVE randomised controlled trial (Robert et al., The Lancet, 2025) demonstrated SADI produced superior weight loss versus Roux-en-Y gastric bypass at 2-year follow-up with a similar safety profile.
A 2025 systematic review and meta-analysis (Sabatella et al., Obesity Surgery) found SADI produced 3.48 times higher odds of type 2 diabetes remission compared to Roux-en-Y gastric bypass — a striking metabolic advantage that makes SADI particularly relevant for patients with advanced or poorly controlled diabetes.
How SADI Differs From Sleeve
The sleeve alone works on restriction and hunger hormone reduction. SADI does all of that and adds a reduction in calorie absorption from fat. Patients eat less, absorb fewer fat calories, and experience a stronger hormonal response which also includes an enhanced GLP-1 signaling from the gut itself, which drives deeper metabolic change. SADI patients typically achieve 70 to 90% excess body weight loss, with stronger long-term durability than sleeve alone.
SADI also preserves the pyloric valve which is the natural passage between the stomach and duodenum which reduces the risk of dumping syndrome that is more commonly associated with traditional gastric bypass. This is a meaningful quality-of-life advantage.
Indications for SADI
SADI is best suited for patients with a BMI of 40 or higher, severe or poorly controlled type 2 diabetes, metabolic syndrome with multiple comorbidities, or inadequate results after a prior sleeve gastrectomy. It is also the most effective revision option available for sleeve patients who need more when the sleeve component is already in place, and the revision adds the intestinal bypass component. In fact this is the preferred revision for weight loss.
Because SADI reduces fat absorption, long-term supplementation of fat-soluble vitamins (A, D, E, K), vitamin B12, iron, calcium, and zinc is essential. Routine lab monitoring is a non-negotiable part of long-term care after SADI.
Which Option May Be Right for You?
Consider GLP-1 Medications if you:
Are not yet a candidate for surgery but want to begin losing weight
Want to reduce surgical risk by losing weight before bariatric surgery
Prefer a non-surgical approach and understand the long-term commitment required
Have a lower BMI and are not yet at surgical candidacy thresholds
Are using medication as a bridge while preparing for a more permanent intervention
Consider Gastric Sleeve if you:
Have a BMI in the 30–49 range
Have earlier-stage metabolic disease or type 2 diabetes
Prefer a procedure without intestinal rerouting
Have tried GLP-1 medications and plateaued, developed side effects, or want a permanent solution
Want a one-time intervention rather than ongoing treatment
Are considering surgery as a first step, with SADI as a potential future upgrade if needed
Consider SADI if you:
Have a BMI of 40 or higher
Have severe or poorly controlled type 2 diabetes
Have metabolic syndrome with multiple obesity-related comorbidities
Have already had sleeve surgery with inadequate weight loss or metabolic improvement
Need the strongest and most durable long-term metabolic results available
Want a single procedure that delivers both restriction and meaningful metabolic change in one step
Can Sleeve Patients Be Converted to a SADI, Can Sleeve Patients Take GLP-1?
The short answer is yes.
Gastric sleeve surgery can be converted to SADI at a later date. Because the sleeve component is already in place, the revision adds the intestinal bypass component thus making it a natural and well-suited path. Revision bariatric surgery is more complex than primary surgery due to scar tissue and altered anatomy, which is why selecting an experienced surgeon from the start matters.
Patients who have had sleeve surgery and later want additional metabolic support can also use GLP-1 medications after surgery. Dr. Bonnor evaluates each case individually and does not take a one-size-fits-all approach to long-term management.
Many patients appreciate knowing that the journey is not always linear. Treatment plans can evolve based on how the body responds which is exactly why continuity of care with the same physician matters.
Beyond Weight Loss: The Full Transformation
Significant weight loss changes how the body looks on the outside. Excess skin, shifted contours, and tissue that didn't adapt as quickly as the weight came off are common outcomes after major weight loss. These concerns can affect comfort, confidence, exercise, and quality of life.
At Texas Aesthetics & Bariatrics in Houston, Dr. Bonnor is board certified in both bariatric and cosmetic surgery. Patients who undergo sleeve or SADI surgery can continue working with the same physician for post-weight-loss body contouring including tummy tuck, arm lift, breast procedures, and body contouring procedures .
This continuity of care is one of the most meaningful differentiators of the practice. One surgeon, the full journey.
Explore Your Options in Houston, TX
Choosing between gastric sleeve, SADI, and GLP-1 medications is a decision that deserves honest, individualized guidance based on what's most popular or most convenient.
At Texas Aesthetics & Bariatrics, located at 18211 Katy Freeway, Suite 250, Houston, TX, Dr. Ricardo Bonnor reviews each patient's full medical profile and helps them understand which option best fits their health history, metabolic needs, and long-term goals. We accept Aetna, United Healthcare, Cigna, and Blue Cross Blue Shield. Self-pay gastric sleeve surgery starts at $9,900 with financing available.
Contact us today to schedule your consultation and get a clear, direct answer about which path is right for you.
FAQs
-
Yes, an increasing number of patients pursue sleeve or SADI surgery after reaching a plateau on semaglutide or tirzepatide, or because they no longer want to manage the ongoing cost and commitment of medication. Prior GLP-1 use often satisfies the documented weight loss attempt requirement many insurance plans require before approving bariatric surgery. Dr. Bonnor's team can help you transition safely from medication to surgery.
-
Neither is universally better. The question should be which one is more appropriate for you and that depends on your medical condition and your goals. Sleeve is the right choice for many patients with BMI in the 30–49 range and earlier metabolic disease. SADI-S is the stronger option for patients with BMI 50 or higher, advanced type 2 diabetes, or those who need more durable long-term results. The important thing to know is that a sleeve can be converted to SADI making a sleeve a natural first step for patients who are unsure.
-
Research consistently shows significant weight regain. A 2025 meta-analysis (Berg et al., Obesity Reviews) found patients stopping semaglutide or tirzepatide regained a mean of 9.69 kg. Most patients return to their pre-treatment weight within approximately 18 months of stopping. This is the fundamental limitation of GLP-1 therapy.
-
Over two years, bariatric surgery patients spent approximately $11,689 less than GLP-1 patients, according to a 2025 JAMA Surgery study of 30,458 patients. Surgery is a one-time cost. GLP-1 medications are an ongoing monthly expense. Self-pay gastric sleeve surgery at Texas Aesthetics & Bariatrics starts at $9,900 with financing available.
-
Yes. Surgery works through a completely different mechanism. Patients who have tried GLP-1 medications and found them insufficient are often strong candidates for bariatric surgery.
-
Yes, SADI requires more vigilant nutritional monitoring than either sleeve surgery or GLP-1 medications because it reduces fat absorption, which also reduces absorption of fat-soluble vitamins (A, D, E, K), vitamin B12, iron, calcium, and zinc. Lifelong supplementation and routine lab work are non-negotiable after SADI. Sleeve surgery requires standard bariatric vitamin supplementation. GLP-1 medications require only standard multivitamins.
-
SADI consistently produces the strongest and most durable type 2 diabetes outcomes. A 2025 meta-analysis (Sabatella et al., Obesity Surgery) found SADI-S produced 3.48 times higher odds of diabetes remission compared to Roux-en-Y gastric bypass. For patients with advanced or poorly controlled diabetes, SADI is often the most appropriate surgical choice. Gastric sleeve also improves diabetes significantly and may be appropriate for patients with earlier-stage metabolic disease.
-
Texas Aesthetics & Bariatrics accepts Aetna, United Healthcare, Cigna, and Blue Cross Blue Shield (BCBS). Coverage eligibility depends on your specific plan, BMI, and documented medical criteria. Prior GLP-1 use may help satisfy insurance documentation requirements. Dr. Bonnor's team reviews your coverage during consultation and helps patients understand options before moving forward.
Clinical References
The following peer-reviewed studies inform this content. All citations are verifiable in PubMed or the original journal.
1. Berg A, et al. Discontinuing glucagon-like peptide-1 receptor agonists and body habitus: A systematic review and meta-analysis. Obesity Reviews. 2025. DOI: 10.1111/obr.13929.
Meta-analysis of 8 RCTs (2,372 participants). Patients stopping semaglutide or tirzepatide regained a pooled mean of 9.69 kg, with weight regain proportional to original weight lost.
2. Brown A, et al. Head-to-head real-world comparison of bariatric surgery vs GLP-1 receptor agonists. Presented at the ASMBS 2025 Annual Scientific Meeting. June 17, 2025. NYU Langone Health / NYC Health + Hospitals.
Real-world study of 51,085 patients with BMI ≥35. Bariatric surgery produced 5× more weight loss than GLP-1 medications at 2 years (58 lbs vs 12 lbs; 24% vs 4.7% total weight loss). Up to 70% of patients discontinued GLP-1 treatment within one year.
3. Sabatella L, et al. Comparison Between SADI-S and Roux-En-Y Gastric Bypass in Terms of Weight Loss, Associated Medical Problems Remission, and Complications: A Systematic Review with Meta-Analysis. Obesity Surgery. 2025. DOI: 10.1007/s11695-025-08092-0. PMC12457536.
Meta-analysis of 8 comparative studies. SADI-S produced 3.48× higher odds of type 2 diabetes remission (OR 3.48; 95% CI 2.02–6.02; p<0.001) and significantly greater total weight loss vs Roux-en-Y gastric bypass.
4. Robert M, Poghosyan T, Romain-Scelle N, et al. Efficacy and safety of SADI-S versus Roux-en-Y gastric bypass (SADISLEEVE): a randomised, open-label, superiority trial at 2 years. The Lancet. 2025;406(10505):846–859. DOI: 10.1016/S0140-6736(25)01070-0.
The first-ever multicentre RCT comparing SADI-S to Roux-en-Y gastric bypass. SADI-S demonstrated superior weight loss at 2 years with a similar safety profile.
5. Barrett T, Hafermann J, Richards S, et al. Obesity Treatment With Bariatric Surgery vs GLP-1 Receptor Agonists. JAMA Surgery. November 2025. PMC12444648.
Retrospective cohort of 30,458 patients. Bariatric surgery produced 28.3% total weight loss vs 10.3% for GLP-1s at 2 years. Bariatric surgery saved approximately $11,689 in ongoing costs over 2 years compared to GLP-1 therapy.
† Berg et al., Obesity Reviews, 2025 (reference 1). ‡ Sabatella et al., Obesity Surgery, 2025 (reference 3). § Barrett et al., JAMA Surgery, 2025 (reference 5).